
Millions of Americans are taking Ozempic, Wegovy, or Mounjaro. Here’s what the data actually says about muscle loss on GLP-1 and how to protect yourself.
Imagine this: You’ve been on semaglutide (Wegovy) for six months. You’ve lost 22 pounds. Your doctor is happy. But lately, getting up off the couch feels harder than it used to. Climbing a flight of stairs winds you. You start to wonder: is this drug taking my muscle along with my fat?
It’s one of the most common concerns people have about GLP-1 drugs. And it’s a fair question. But the full answer is more nuanced than the scary headlines suggest.
This guide breaks down why does GLP-1 cause muscle loss, who is truly at risk, and what you can do starting today to protect your muscle while losing fat.
What Do GLP-1 Drugs Actually Do?
GLP-1 stands for Glucagon-like peptide-1. It’s a hormone your body already makes naturally, usually after you eat. These drugs either mimic that hormone or boost it.
Think of it this way: your gut sends a “I’m full” signal to your brain. GLP-1 drugs make that signal louder and longer-lasting. The result? You eat less, feel full sooner, and your stomach empties more slowly.
- Appetite suppression: Signals the brain’s hunger center (hypothalamus) to reduce cravings
- Gut slowing: Food moves through your stomach more slowly, keeping you full longer
- Blood sugar control: Originally developed for type 2 diabetes before weight loss benefits were discovered
- Weight loss mechanism: The calorie deficit created by eating less is what drives fat loss
Quick note on natural GLP-1 boosters: Certain foods and drinks, like Yerba Mate, can mildly raise your GLP-1 levels naturally. But prescription drugs like semaglutide (Ozempic/Wegovy) produce a far stronger and more sustained effect.
Common brand names in the U.S. include:
- Ozempic and Wegovy (both semaglutide)
- Mounjaro and Zepbound (tirzepatide)
- Victoza (liraglutide)
Each works on the same basic principle but with different strengths and targets.
The Real Numbers: How Much Muscle Do People Lose?
If you are searching questions like does Ozempic cause muscle loss? Does Wegovy cause muscle loss? Or does Tirzepatide cause muscle loss? We will try to explain this through clinical trials.
In any kind of weight loss, whether from dieting, surgery, or medication, some lean mass is typically lost alongside fat. Researchers call this the “quarter rule”: in lifestyle-based weight loss, roughly 25% of the weight you lose tends to be lean mass (everything that’s not fat or bone).
Here’s how GLP-1 drugs compared:
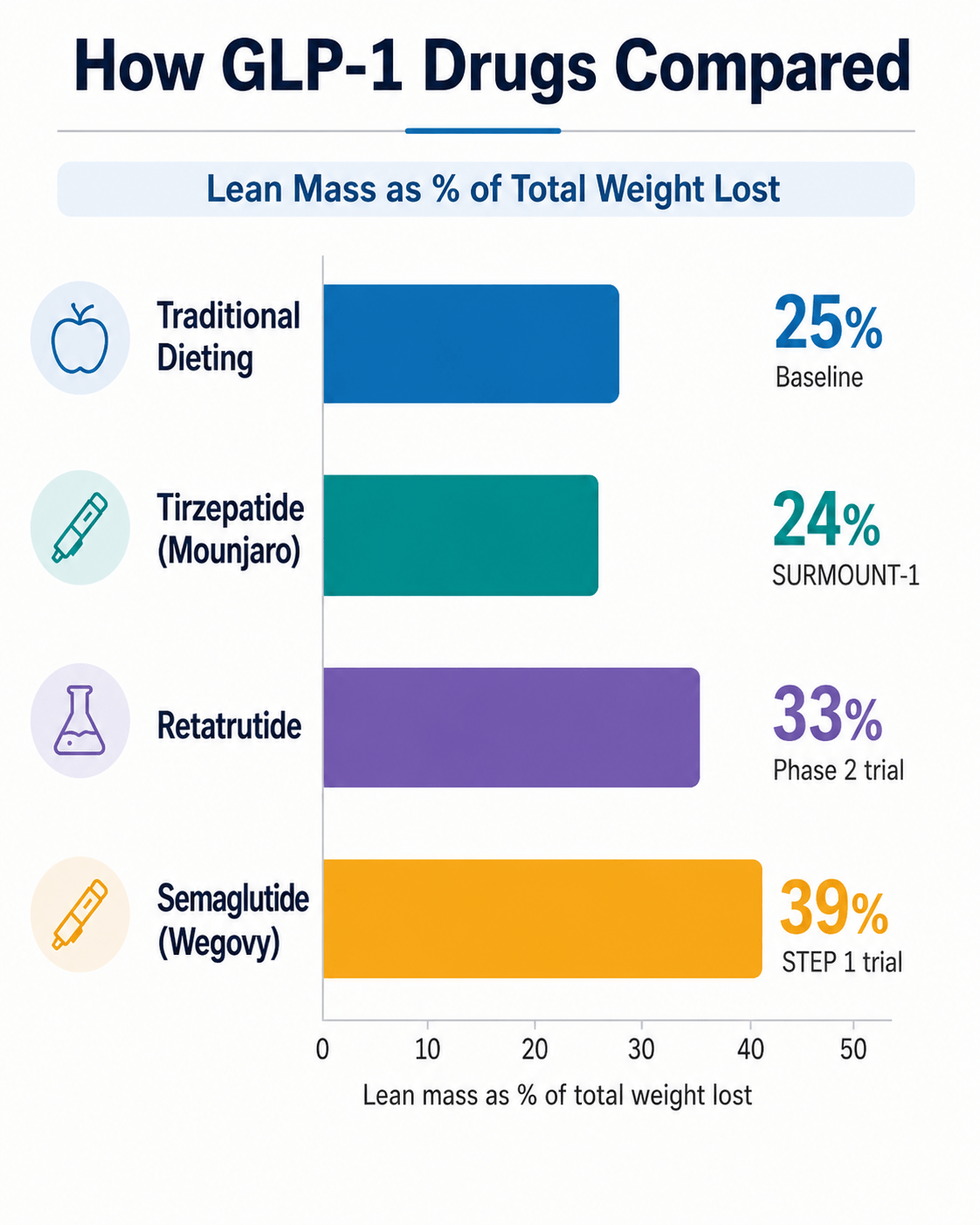
At first glance, semaglutide’s 39% looks alarming. But there’s a major reason these numbers are misleading.
Why DEXA Scans Overstate Muscle Loss
DEXA scans (a common body composition test available at many gyms and clinics across the U.S.) measure body fat, bone, and “lean mass.” The problem is that lean mass is not the same thing as muscle.
Lean mass on a DEXA scan includes:
- Actual skeletal muscle
- Water and fluid stored in tissues
- Glycogen (stored carbohydrate in muscles and liver)
- Intramuscular fat (fat stored inside and around muscle tissue)
When people with obesity lose weight, they also lose the fat that’s been sitting inside their muscles. This is called myosteatosis (myo = muscle, steatosis = fat buildup). The DEXA scan counts this fat loss as “lean mass loss” but losing that fat is actually a good thing for your metabolic health.
Think of it like cleaning out a clogged pipe. Removing fat from inside a muscle doesn’t weaken it, rather makes the muscle work more cleanly and efficiently. DEXA can’t tell the difference between losing muscle fiber and losing intramuscular fat, so it reports both as “lean mass lost.”
| Drug | Trial | Total Weight Lost |
Lean Mass Lost (%) |
Note |
|---|---|---|---|---|
| Semaglutide (Wegovy) |
STEP 1 | ~15% | ~39% | Includes fluid, glycogen loss |
| Tirzepatide (Mounjaro/Zepbound) |
SURMOUNT-1 | ~22% | ~24% | Closest to natural diet benchmark |
| Retatrutide | Phase 2 | ~24% | ~33% | Newer triple agonist, less data |
| Traditional dieting | Multiple studies |
Varies | ~25% | Standard comparison benchmark |
Does Losing Lean Mass Mean Losing Strength?
Here’s where things get interesting (and reassuring).
In the semaglutide trials, patients who lost lean mass on DEXA actually showed a 4.5 kg improvement in hand grip strength over 12 months. And that was without any structured exercise program. How is that possible?
The Hiking Pack Analogy
Imagine you’re hiking a trail in the Rocky Mountains with a 40-pound pack on your back. Now imagine someone removes 15 pounds of rocks from that pack. You didn’t get stronger. But suddenly the trail feels much easier. Your legs aren’t getting stronger; they are just carrying less weight.
That’s what happens when someone with obesity loses body fat. The same amount of muscle is now moving a lighter body. The result often feels like getting stronger, even if muscle volume didn’t change.
Muscle Quality Matters Too
Researchers are starting to measure force output per unit of muscle, not just muscle size. When intramuscular fat is removed, the muscle works more efficiently. This means you can get functionally stronger even as your DEXA “lean mass” number goes down.
A few other improvements seen in GLP-1 users include:
- Better VO2 max which is important for everyday endurance, like walking upstairs or keeping up with kids
- Reduced prevalence of sarcopenic obesity (having both obesity and low muscle mass) from 49% to 33% in semaglutide data
- Improved mobility and balance as joint load decreases
The key distinction: Scale muscle mass (what DEXA measures) went down slightly.
Functional strength (what you can actually do) often went up. For most people, the second number is the one that matters for quality of life
Who Should Actually Be Worried about GLP-1?
Muscle loss is not a concern everyone on GLP-1s faces equally. There are specific groups who are at genuinely higher risk of real, functional decline.
Adults Over 60: Natural age-related muscle loss (sarcopenia) accelerates the impact of any additional lean mass reduction.️
Sedentary Individuals: Without regular movement, the body has no reason to preserve muscle during a calorie deficit.
Low Baseline Muscle Mass: If you’re already low on muscle, even a small additional loss can push you into functional impairment.
Severe Nausea: A common side effect that leads to under-eating protein, which is the main fuel for maintaining muscle.
Two Additional Risk Factors That Don’t Get Enough Attention
Rapid dose escalation: When patients rush through their dose increases too quickly to lose weight faster, the calorie restriction becomes very aggressive. The body loses weight faster than diet, and exercise can compensate for, and a larger share of that weight ends up being muscle.
Stopping the drug and restarting: When people stop GLP-1 medications and regain weight, that regained weight is mostly fat, not muscle. Each stop-start cycle can leave you with a progressively worse body composition, even if the scale goes back to the same number.
Warning signs to take seriously: Difficulty getting up from a chair without using your arms, struggling on stairs you used to manage easily, or a noticeable drop in your gym performance are signs your muscle loss may have gone beyond the adaptive range. Talk to your doctor.
How to Prevent Muscle Loss on GLP-1?
The good news: most muscle loss on these medications is preventable. Here’s a practical plan.
1. Prioritize Protein at Every Meal
Aim for 1.2 to 1.6 grams of protein per kilogram of body weight per day. For a 200-lb American adult, that’s roughly 109 to 145 grams of protein daily. Spread it across meals, targeting 25 to 40 grams per sitting. For example,
- Eggs and Greek yogurt at breakfast
- Grilled chicken at lunch
- Salmon or a protein shake at dinner.
If nausea is making eating hard, a high-quality protein shake can help you hit your target without forcing a full meal.
Read More: Rethinking Protein: Exploring Plant-Based Alternatives for a Healthier, Sustainable Diet
2. Do Resistance Training (This Is Non-Negotiable)

Lift weights, use resistance bands, or do bodyweight exercises at least 2 to 4 times per week. Resistance training sends a direct signal to your body to keep the muscle it has, even in a calorie deficit.
Studies show it can cut lean mass loss by nearly 50%. You don’t need a gym membership. Exercises like squats, push-ups, lunges, and planks at home count. Even starting with two 30-minute sessions per week makes a significant difference.
Also Read: Thinking Weightlifting isn’t for you? You Might Be Surprised
3. Don’t Cut Calories Too Aggressively
Target a steady loss of 0.5% to 1% of your body weight per week. For a 200-lb person, that’s about 1 to 2 lbs per week. Dropping below 800 to 1,000 calories per day dramatically increases muscle breakdown.
The drug is already creating a deficit for you. There’s no need to also drastically restrict food. Eating too little on top of the medication is one of the most common mistakes people make.
4. Protect Your Recovery

Sleep and hydration directly impact whether your body repairs or breaks down muscle. Aim for 7 to 9 hours of sleep per night. Poor sleep raises cortisol (a stress hormone), and high cortisol is a known trigger for muscle breakdown. Staying well hydrated also helps maintain the glycogen stores in your muscles, which DEXA reads as lean mass.
5. Track Strength, Not Just Body Weight
The number on the scale doesn’t tell you whether you’re losing fat or muscle. Better metrics to track include:
- Can you do more push-ups than last month?
- Is your grip strength holding steady?
- Are daily activities like carrying groceries or climbing stairs getting easier?
If you have access to a DEXA scan, tracking it every 3 to 6 months is useful.
Protein Target Quick Reference
| Body Weight (lbs) | Body Weight (kg) | Min Protein (1.2 g/kg) |
Max Protein (1.6 g/kg) |
|---|---|---|---|
| 150 lbs | 68 kg | 82 g/day | 109 g/day |
| 175 lbs | 79 kg | 95 g/day | 127 g/day |
| 200 lbs | 91 kg | 109 g/day | 145 g/day |
| 225 lbs | 102 kg | 122 g/day | 163 g/day |
| 250 lbs | 113 kg | 136 g/day | 181 g/day |
What the Research Still Doesn’t Know
Being honest about the limits of current evidence is important. Here’s what scientists are still working out:
Long-term data
Most trials run 68 to 72 weeks. We don’t yet know how body composition changes beyond 2 to 3 years of continuous use.
Diverse populations are underrepresented
Trial participants skewed toward certain age groups and ethnicities. Results may look different across the broader U.S. population.
Newer drugs have less data
Retatrutide (the “triple agonist”) and oral options like orforglipron are still in early trials. Muscle data is limited.
No GLP-1-specific protein standard
There’s no consensus yet on whether people on GLP-1s need more protein than the standard dietary guidance suggests.
“The drug handles the deficit. What you do alongside it shapes the composition of the outcome.”
The Bottom Line
Some lean mass loss on GLP-1 drugs is real. But most of the scary numbers you’ve heard are inflated by measurement limitations, and the functional impact is often the opposite of what people fear.
If you add resistance training and hit your protein targets, the research suggests you can cut lean mass loss by nearly half — and come out of the weight loss period with a stronger, leaner, more metabolically healthy body.
The bigger risk isn’t the medication. It’s taking the medication passively, without the lifestyle habits that protect your muscle along the way.
Before starting or adjusting any GLP-1 medication, talk with your doctor or a registered dietitian. A personalized plan will always outperform a general one.
Interested in blogs related to health and fitness, read our other blogs covering physical strength, mental health practices, and different types of diet at Stay Healthy and Stay Fit.
NOTE: This blog is only for educational purpose. Please don’t consider this a treatment procedure. Please contact doctors or medical experts for safest and most effective results.
FAQs
1. Can you regain muscle after losing weight on GLP-1 drugs?
Yes. Muscle can be rebuilt with consistent resistance training, enough protein, and proper recovery. The process may take time, especially for older adults or people who were inactive before starting treatment.
2. Are smart scales accurate for tracking muscle loss?
Smart scales can show trends, but they are not highly accurate for measuring muscle changes. Hydration, food intake, and time of day can affect readings. Use them as a rough guide, not a medical-grade measurement.
3. Should people on GLP-1 drugs take creatine?
Creatine may support strength and muscle performance for some people, especially when combined with resistance training. However, anyone with kidney issues or existing medical conditions should check with a doctor first.
4. Can vegetarians or vegans protect muscle while using GLP-1 drugs?
Yes. Plant-based protein sources like tofu, tempeh, lentils, chickpeas, soy milk, edamame, pea protein, and seitan can help meet protein needs when planned properly.
5. When should someone speak to a doctor about weakness on GLP-1 drugs?
Speak to a doctor if weakness feels sudden, daily tasks become harder, dizziness or severe nausea persists, or exercise performance drops sharply. These signs may need medical review.